

Chest Reconstruction Top Surgery and Drains
This article provides information on the function, risks and benefits of surgical drains in the hope of addressing the increased confusion and anxiety surrounding this topic. Generally speaking, our surgeons try to give surgical drains to all top surgery patients, and especially those that are at a heightened risk for hematomas: patients with high levels of body fat, patients who undergo liposuction and/or patients who have significant amounts of tissue removed. We also discuss common concerns around surgical drains such as pain, discomfort, seromas, and their effect on your top surgery scars.
Are Drains Necessary?
The question of whether or not to use drains has increased confusion and anxiety about surgery perhaps more than any other top surgery topic. Rest assured that drains are not bad, and the stakes for using them (slight pain and annoyance) are not as high as they are made out to be.
At The GCC (Gender Confirmation Center), the patient generally gets to decide if they prefer drains for double incision surgeries; however, drains are required for other procedure types such as keyhole and periareolar surgeries.
What Are Drains and Why Are They Used?
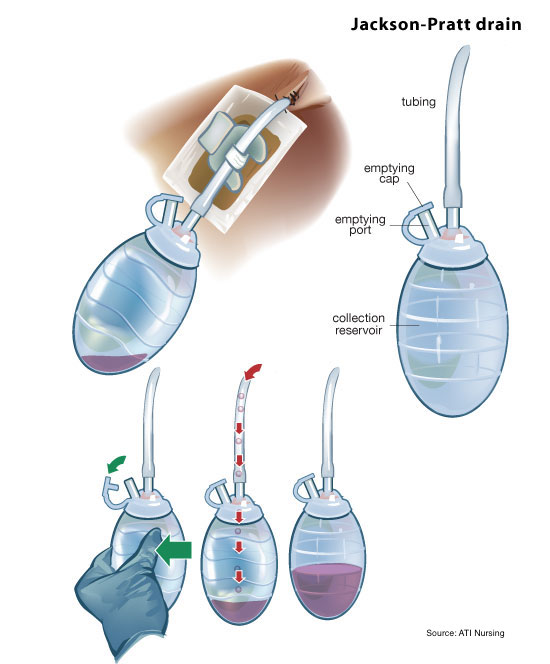
The Jackson-Pratt (JP) drain is a medical device more commonly referred to in the top surgery world simply as ‘drains.’ The device draws out fluid that collects under your incisions after your surgery. Drains are very effective to reduce the risk of having a fluid collection under the skin after surgery, also called a seroma, or the collection of blood around wounds, called a hematoma.
Seromas After Surgery
All of our surgeons’ chest reconstruction top surgery techniques involve meticulous chest contouring. To ensure that the contours on the upper chest and sides are smooth and uniform, our surgeons use a technique called undermining (WARNING: the link contains a graphic intraoperative photo). When a lot of undermining is performed, there’s a possibility that the area can fill with fluid after surgery. The ‘fluid’ is exactly like the fluid that would appear on your knee if you skinned your knee very hard. It is one of the ways the body heals. Sometimes there is enough fluid produced into a healing area that it becomes a pool of fluid under the incisions; this is what we call a seroma. A seroma is not a serious complication, but it can be an inconvenience during your recovery.
Treatment of small seromas: A small seroma doesn’t always require medical treatment. The body may naturally reabsorb the fluid in a few weeks or months. However, even small seromas will lead to much longer swelling in the area of weeks to months.
Treatment of larger seromas: If a larger seroma develops it may require drainage of the seroma in the doctor’s office. This process is completed by numbing the skin, inserting a needle and drawing out the fluid. It can take 2-4 weekly visits to get to the point that a seroma will not return.
Consequences of a seroma: Seromas can be tight, uncomfortable, and they can delay the disappearance of your swelling by weeks or months. However, seromas are not likely to change your final outcome.
Prevention of seromas: The chance of having a seroma can be greatly reduced by utilizing drains and compression garments.
Pros and Cons of Drains
Why don’t people like drains?
The placement of drains may cause additional scarring and pain, which is where the stigma against drains originates. However, our surgeons’ techniques do not cause any additional scarring. The only visible scarring that may result from drains would be very small scars under the arms for someone undergoing a minimally-scarring procedure, such as the periaerolar top surgery. Drains produce no additional scarring at all for patients who opt for double incision, buttonhole or fishmouth procedure types. The discomfort that drains cause are minimal and the benefits greatly outweigh the inconveniences.
Do they hurt?
The placement of drains is intended to limit discomfort, healing complications, and scarring. The way our surgeons place the drains usually makes them pain free, or they may cause only minor temporary discomfort.
Do they cause extra scarring?
As mentioned above, there are no extra incisions for the drainage tubes for those who undergo a double-incision, buttonhole or fishmouth top surgery. Instead, the tubes exit the chest from the outer part of the already existing chest incision. For a procedure with minimal scarring (eg, periareolar or keyhole), there will only be very small scars under the arms, right below the armpits, from where the drains are inserted.
Making The Final Decision
How do drains work?
When the bulb is compressed (squeezed) with the stopper in place, a constant gentle suction is created. In order for the drain to draw fluids away from the surgical site, the bulb should be compressed at all times (unless you are draining the fluids).
How to empty your drains?
- About 2-3 times a day, the fluid will need to be emptied from the reservoir. Your medical team will show you how to strip your tubing and empty your drain system.
- The fluid will be emptied into a cup that is marked with milliliters. Record the ml amount each time using this drain log PDF.
- After emptying the fluid, remember to squeeze the bulb until it is flat and place the stopper into the bulb. This action creates the suction needed to draw out the body fluid.
Who should empty your drains?
- Either you, or someone who is caring for you, can empty the drains. It should take about 15-30 seconds per drain. The nurse will teach you to do this before you leave the surgery center or hospital.
What should my fluid look like?
- The color of the fluid is not important. It is usually bloody in the beginning with a dark red appearance.
- As your incisions heal, the fluid changes to light pink, then yellow, and finally clear.
When can I get my drains removed?
Typically, drains are taken out when the fluid output remains below 30 ml for two consecutive days. In most cases, this removal occurs between the sixth and seventh day following surgery. The process of removing drains is usually not associated with significant discomfort; many individuals simply describe it as a somewhat unusual sensation. This sensation originates from inside the chest, so applying numbing cream to the skin site would not alleviate it. If patients have concerns about this, they can discuss them with their healthcare provider during a preoperative or postoperative appointment to receive further reassurance.
Contact us if any of the following occurs:
- Fever greater than 101F
- Bulb doesn’t hold suction (make sure the emptying cap is closed securely)
- Tubing falls out of the body
Learning by Video!
We created this helpful video about how to manage your drains if that might be of assitance to you as you prepare for surgery
Final Thoughts on Drains
We usually recommend our patients opt for drains. They will help you have the most reliable recovery possible. If you do opt for drains for double incision, remember that there are no extra incisions for the drainage tubes. Drains do not usually add any or very minor discomfort, and we believe they are well worth it for an expedited healing process.
Request a Free Surgical Consultation Today.
All virtual and in-person consultations with our board-certified surgeons are free. Once you fill out this form, our patient care team will reach out and guide you through every step to get to surgery.
Suite 1010, 450 Sutter St
San Francisco, CA 94108
Phone: (415) 780-1515
Fax: (628) 867-6510
GCC business hours are from 9:00 am to 5:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
Board Certification
& Memberships

![]()
![]()
Copyright © 2023 GCC (Gender Confirmation Center). All Rights Reserved.