

Metoidioplasty and Phalloplasty: Options for Masculinizing Bottom Surgery
Medically reviewed by Ellie Zara Ley, MD on February 6, 2024.
Transmasculine and Nonbinary individuals can sometimes feel a sense of incongruence with their natal genitalia–meaning the genitalia that they were born with. This feeling is frequently referred to as bottom dysphoria, and influences how trans-masculine people move through the world. Some patients express that these feelings are particularly distressing in moments of intimacy or while using the bathroom. Masculinizing techniques for bottom surgery, also known as “FTM” bottom surgery can help alleviate these feelings. The two methods available are metoidioplasty and phalloplasty, often referred to as “meta” and “phallo”. While both of these procedures will create a penis, they vary in aesthetics, sensitivity and function. A metoidioplasty is a procedure that releases the natal erectile tissue, sometimes called a clitoris, from surrounding ligaments to appear more prominent as a penis. A phalloplasty creates a penis from a flap of skin taken from the forearm, groin, or thigh.
We will dive into the differences between the two so you can gain a better understanding of which procedure best fits your goals. The following information is important to consider when contemplating the two procedures.
Metoidioplasty: Procedure Details
The metoidioplasty procedure involves releasing the natal erectile tissue, sometimes called the clitoris, from its surrounding ligaments. An incision is made at the base of the glans of the penis/clitoris and surrounding skin is pulled back. The labia minora can be left intact or completely removed. A simple metoidioplasty ends at this stage, giving the penis a more prominent and forward position on the body. On the other hand, a metoidioplasty with primary urethral lengthening (PUL) will extend the urethra so that it ends at the tip of the penis shaft. This allows patients to urinate while standing up.
The recovery process for a metoidioplasty is shorter and less involved than a phalloplasty. A metoidioplasty cannot create a penis of girth and length; while some patients are satisfied with this, others may desire more. Having a metoidioplasty does not exclude the possibility of getting a phalloplasty in the future. In fact, due to BMI requirements, many patients who want a phalloplasty will start with a metoidioplasty as the first stage of their gender surgery, while working on weight loss.
Phalloplasty: Procedure Details
A phalloplasty is a multistage procedure. The number or stages depends on your goals and the type of phalloplasty you choose to undergo. Initially, a penis is constructed using a flap from the forearm, the groin or the thigh. These procedures are called the Radial Forearm Free (RFF) Flap, the anterolateral thigh flap (ALT) and groin flap phalloplasties. Patients who undergo phalloplasty can undergo the following additional procedures, either during the initial surgery or in a later stage:
- Urethral lengthening
- Scrotum creation, insertion of scrotum expanders and eventually testicular implants.
- Vaginectomy or the closure of the vaginal canal
- Glansplasty or the creation of a glans
- Insertion of erectile device
- Mons Resection
Choosing Between Metoidioplasty and Phalloplasty
When considering metoidioplasty versus phalloplasty, several key factors come into play. We discuss them in depth in the sections below.
- Sensitivity: If being able to experience heightened, erotic sensitivity in your penis is a high priority, a simple metoidioplasty, metoidioplasty with PUL, an RFF and/or ALT phalloplasty may be a good fit for you.
- Urinate standing up: If being able to urinate standing up is a high priority, undergoing a metoidioplasty or phalloplasty with a primary urethral lengthening may be a good fit for you. That said, undergoing this procedure requires a simultaneous vaginectomy with Dr. Ley.
- Penis length: If having a penis that is greater than 3 inches in length is a priority, a phalloplasty may be a better fit for you than a metoidioplasty.
- Number of surgeries and recovery length: If you would like to minimize the amount of surgeries you have to go through, a metoidioplasty may be a better fit for you than a phalloplasty. That said, the groin flap phalloplasty involves more surgical stages to construct than the other phalloplasties: RFF and ALT.
- Scar visibility: If having no visible scars or being able to easily conceal your scars is a high priority, a metoidioplasty or groin flap phalloplasty may be a greater fit for you than an RFF or ALT phalloplasty.
- BMI limitations: If your BMI is over 32, you may not qualify for an ALT phalloplasty. If your BMI is over 30, you may not qualify for a RFF or groin flap phalloplasty. If your BMI is over 35, you may not be eligible for metoidioplasty with primary urethral lengthening. If your BMI is over 40, you may not qualify for a simple metoidioplasty. These limitations are based on the high risk of complications. Patients outside of these BMI ranges may choose to undergo a metoidioplasty or a mons resection as a first stage procedure while working to lower their BMI in order to qualify for their desired procedures.
- Insurance and costs: The financial implications, including the cost of the procedures and the availability of insurance coverage, should be thoroughly evaluated. Generally speaking, metoidioplasty procedures are less costly than a phalloplasty, especially since the latter is more likely to involve multiple stages of surgery to achieve the final result. The GCC (Gender Confirmation Center) is only able to offer phalloplasty and metoidioplasty with PUL to patients with health insurance at this time. The GCC’s free insurance concierge service has a 90% success rate of securing coverage for interested patients.
Key Procedure Differences: Metoidioplasty vs. Phalloplasty
Scarring
The RFF and ALT phalloplasty procedures are notorious for leaving behind more visible scars on the body than a groin phalloplasty or metoidioplasty. Patients who do not want visible surgical scars often opt for the latter two procedures.
A phalloplasty involves taking a skin graft from a different part of the body to construct a penis. These are commonly from the forearm (RFF phalloplasty), thigh (ALT phalloplasty) or groin. Patients will have a large rectangular scar which will be visibly discolored compared to the surrounding skin. While the groin phalloplasty scar is the least visible, forearm and thigh scars can also be concealed with clothing. Patients can also opt for re-pigmentation of the scar with a medical tattoo provider a year after recovery.
Metoidioplasty, on the other hand, leaves behind very little scarring. Some scarring may occur from urethral lengthening or creation of a scrotum. If minimal scarring is essential, metoidioplasty may fit your aesthetic goals.
Urination
For many transmasculine and nonbinary individuals, urinating while standing is a goal of bottom surgery. This is because peeing standing up can relieve dysphoria and make some patients feel safer using public restrooms.
Standing to void or urinate can be achieved with both a metoidioplasty and phalloplasty, although a simple metoidioplasty or first stage phalloplasty will not allow you to urinate standing up. A primary urethral lengthening (PUL) will lengthen the urethra and to the end of the penis shaft. This will allow for urination while standing. Note that at GCC, we require that patients undergo a vaginectomy at the same time as a urethral lengthening due to the high risk of urinary complications.
Erogenous Sensation or Genital Sensitivity
The sensation you are left with will depend on the type of procedure you undergo. Since the nerves are not altered during a metoidioplasty, it is very likely that sensation will be the same post-op. A phalloplasty can feel a little different. A groin flap phalloplasty will have tactile sensation, meaning that it will likely not be as sensitive as your clitoris. Alternatively, in the thigh and forearm flap phalloplasty, the clitorial nerve is hooked up to a nerve from the donor site, which means that there is a probability of experiencing heightened sensitivity in the penis. Even when the clitoris is buried, it can still be stimulated under the skin. Orgasm is possible with both procedures, and some patients who undergo urethral lengthening have reported being able to ejaculate clear fluid upon orgasm.
Penetrative Sex
For some patients, a metoidioplasty will generally allow you to experience an erection, as blood flow to erectile tissue is maintained. If you are able to experience an erection with your clitoris/bottom growth after testosterone hormone therapy, you may be able to experience an erection after metoidioplasty. Depending on your healing, about three months after a metoidioplasty, patients may use penis pumps to enlarge the size of their penis, which may help with penetration.
Phalloplasty offers a higher likelihood of achieving penetrative capability, as the resulting penis size is typically larger. Sexual activity after surgery varies based on the type of phalloplasty, the number of stages, and the individual’s healing process. The constructed penis does not achieve natural erections; however, patients can use silicone erectile sleeves or, after a year, consider a procedure to implant an erectile device, such as a saline pump or a flexible rod. While these devices don’t change the overall size, they can slightly increase the penis’s girth.
Penis Size
Phalloplasty allows for a phallus of average size. That said, the final size and girth is greatly dependent on the amount of donor tissue available.
Metoidioplasty results will depend on the size of your bottom growth from testosterone therapy. The penis created from a metoidioplasty is generally smaller compared to the result of a phalloplasty. Likewise, undergoing additional procedures like a mons resection or panniculectomy can give the penis a more forward, visually apparent position on the body.
While penis size can be linked to gender affirmation for some individuals, we remind our patients that it does not define one’s sexual function, masculinity, or capacity for erotic sensation.
Additional Procedures
Patients can undergo additional procedures such as scrotoplasty, the insertion of testicular expanders, the insertion of testicular implants, and more. For example, Dr. Ley (she/her/they) can construct a scrotum and insert silicone testicular implants over the course of multiple surgeries for metoidioplasty and phalloplasty patients.
Recovery
Recovery from bottom surgery can be challenging. For many patients, a key factor in choosing between metoidioplasty and phalloplasty is the intensity of the recovery process and the number of surgeries required to achieve their desired outcome.
We encourage you to consider the following factors around recovery when making a decision about which procedures are right for you:
Revisions and Complications
Any complication, even if minor and manageable at home, can feel frustrating and like a setback in recovery. Phalloplasty is a more complex, multi-stage procedure compared to metoidioplasty. Likewise, metoidioplasty with primary urethral lengthening (PUL) is more complex than a standard metoidioplasty. The most common complications with any urethral lengthening are urinary fistulas and wound dehiscence or openings.
As a former patient herself, Dr. Ley (she/her/they) has firsthand experience of the importance of helping her patients achieve their desired bottom surgery results. She is highly sought after within the transgender community for bottom surgery revisions. If you are interested in undergoing surgery with Dr. Ley, you can request a consultation with her here.
Physical and Emotional Impact
Undergoing multiple surgeries often involves both emotional and physical sacrifices. This may include extended recovery times, hospital stays, bed rest, pain, discomfort, inflammation, and periods when sexual activity, including masturbation, is not possible. Not everyone is willing or able to commit to a procedure that demands an extensive recovery.
However, this may not be the case for you. Many patients find that once they can see and enjoy the final results, the pain and discomfort of recovery feel worth it.
If you’re interested in a surgery with a less intensive recovery, metoidioplasty may be preferable. Metoidioplasty recovery is often less demanding, as it requires healing in fewer areas.
Engaging in Sexual Activity
Metoidioplasty patients typically need to wait around 6–8 weeks before attempting oral or manual stimulation of their penis, while phalloplasty patients may need to wait longer. Recovery timelines vary for each patient, so it’s best to consult your surgeon about when it’s safe to resume sexual activity.
Some metoidioplasty patients use a penis pump as a part of their sex lives; patients should wait at least three months after getting a metoidioplasty to start using a pump. Phalloplasty patients who wish to use a penis pump and/or silicone erectile sleeves should consult their surgeon on when they can use these devices. This is because recovery times vary from patient-to-patient and depend on the type of phalloplasty you undergo, how long you have in between procedures and how long it takes to heal from each stage.
Cost and Insurance Coverage
At GCC, our team can guide you through the available cash and insurance options for metoidioplasty and phalloplasty procedures. Additional costs, such as anesthesiology, pathology, or other hospital fees, may apply as add-ons to the procedure cost. For cash pay patients, meaning those who are paying without insurance coverage, a metoidioplasty can cost between $19,000-$42,000. Insurance coverage can help patients significantly reduce these costs. At the GCC, we only perform phalloplasty for patients with insurance coverage due to hospital restrictions. A patient’s deductible for a phalloplasty will vary on a case-by-case basis. To get your quote for surgery, you can start by soliciting a free consultation here.
Although more providers are approving gender affirming surgery, it is essential to review the requirements with your specific insurance provider. Please note that most insurers have more stringent criteria for covering bottom surgery compared to other gender-affirming procedures like top surgery. At GCC, our insurance advocacy team has achieved a 90% success rate in securing coverage for interested patients.
FAQ
What is the primary difference between metoidioplasty and phalloplasty?
The main differences between these procedures lie in the size of the resulting penis, the possibility of preservation of sensation, and the potential for penetrative intercourse. Metoidioplasty releases the existing natal erectile tissue to create a more prominent penis while preserving sensation. In phalloplasty, a penis is constructed using skin and tissue from other parts of the body, such as the forearm, groin, or thigh. Sensory nerves are connected to the phallus as part of the staged procedure, helping enhance sensation.
Which procedure has a shorter recovery time?
A simple metoidioplasty typically involves a shorter recovery time of around 6–8 weeks. However, when metoidioplasty is combined with urethral lengthening, recovery is longer, with patients generally requiring two catheters for 2–3 weeks postoperatively. Swelling should fully resolve within 3–6 months, allowing you to see the final result. Overall, metoidioplasty has a shorter recovery time than phalloplasty due to the less extensive surgical process.
Can I achieve erectile function with both procedures?
Both procedures enable erectile function, but the methods differ. A metoidioplasty preserves all natal sensory nerves, ensuring continued erectile function after surgery. In contrast, phalloplasty involves using tissue from other areas of the body, which require prosthetic implants to achieve an erection. Non-surgical options, such as penis pumps or silicone erectile sleeves can also be used.
What are the potential complications of these procedures?
Minor complications from both metoidioplasty and phalloplasty can usually be managed at home. However, major issues such as urethral strictures, fistulas, infections (though rare), or graft loss will be addressed by your care team. It’s essential to maintain open communication with your team throughout your recovery.
Do I need to have bottom growth to undergo a meta or phallo?
Bottom growth is a term that describes the growth of the natal erectile tissue from testosterone hormone therapy. Not all patients undergoing testosterone hormone therapy experience this effect, and the degree of growth can vary significantly from person to person.This effect is not experienced in all patients who undergo testosterone hormone therapy. Likewise, the amount of growth experienced is different from person to person.
While some surgeons may require patients to undergo 1-2 years of testosterone therapy before a metoidioplasty, Dr. Ley does not have this requirement. It’s important to note that the amount of available genital tissue can contribute to a larger, more prominent surgery result. Additional procedures like a mons resection and panniculectomy can also help give the penis a more forward, prominent position on the body.
Every journey is unique, and testosterone therapy is not a prerequisite for surgery. If you have questions about bottom growth and bottom surgery, you can ask Dr. Ley in a free consultation.
Will I need to undergo hair removal prior to a phalloplasty?
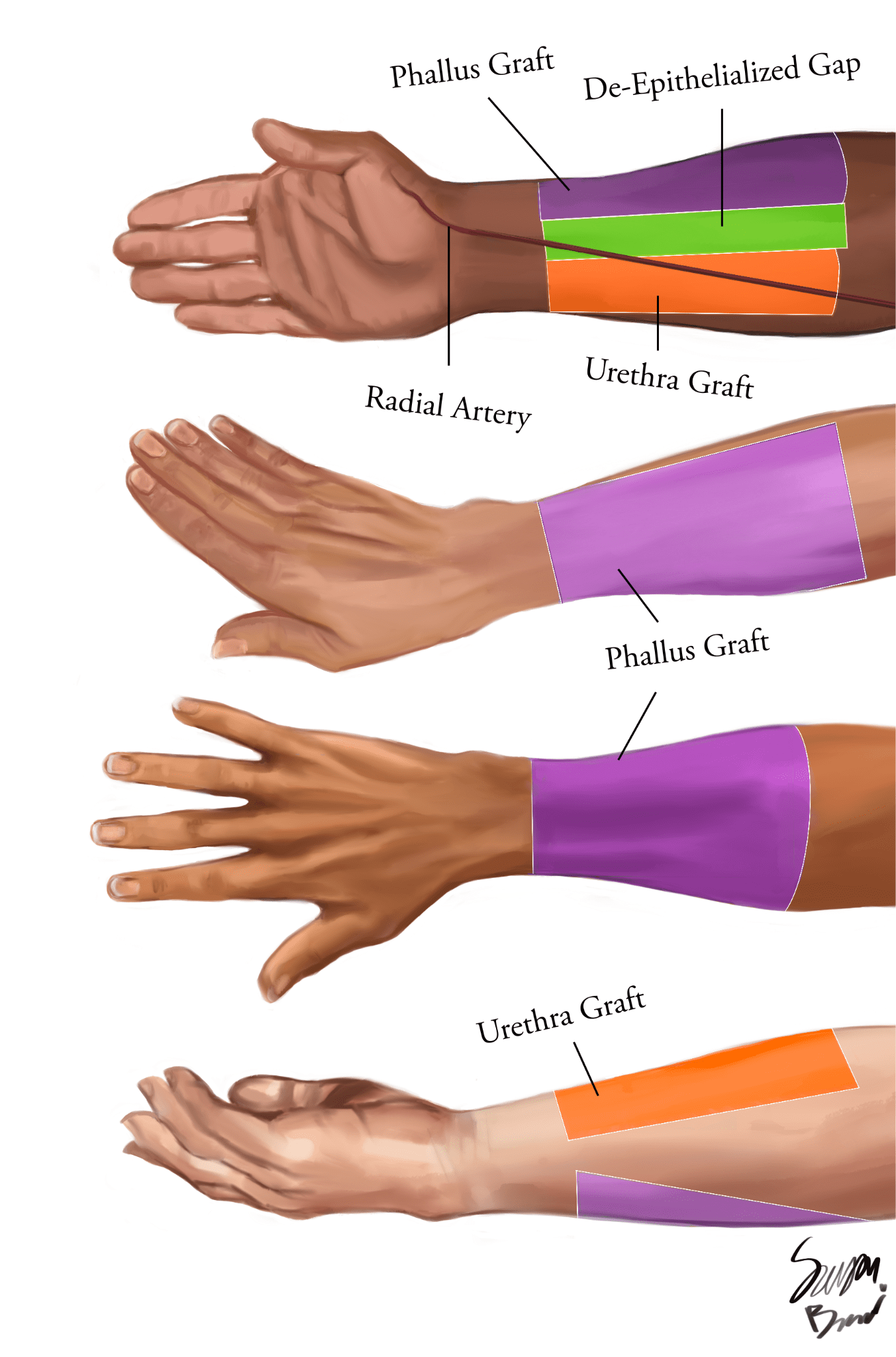
Patients that would like to undergo an RFF phalloplasty or have a urethral graft taken from the forearm must undergo Electrolysis hair removal to this area prior to surgery. Please note that permanent hair removal is only required for the section of the forearm (highlighted in orange on the illustrations) that will be used as a graft to extend the urethra out to the tip of the penis. This is due to the fact that hair growth inside of the urethra can cause a variety of complications. For more information, click here.
Conclusion: How do I determine which procedure is right for me?
Choosing the right procedure is a personal decision that should be based on your individual goals and desired outcomes regarding sensitivity, function, and aesthetics. We also encourage patients to consider potential risks, complications, and their preferences for recovery. Additionally, BMI restrictions on a metoidioplasty with primary urethral lengthening (PUL) and phalloplasty procedures can be a limiting factor for some.
Coming into a consultation informed about these factors, with any questions you may have, will help to foster an open dialogue with your provider to determine the best procedure for you. Ultimately, the decision is yours, and it’s important to make an informed choice about what’s right for you.
Request a Free Surgical Consultation Today.
All virtual and in-person consultations with our board-certified surgeons are free. Once you fill out this form, our patient care team will reach out and guide you through every step to get to surgery.
Suite 1010, 450 Sutter St
San Francisco, CA 94108
Phone: (415) 780-1515
Fax: (628) 867-6510
GCC business hours are from 9:00 am to 5:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
GCC phone hours are from 9:00 am to 4:00 pm
Board Certification
& Memberships

![]()
![]()
Copyright © 2023 GCC (Gender Confirmation Center). All Rights Reserved.